Mortality data during the vaccine roll-out period
Below we republish part of a briefing in the Health Advisory & Recovery Team (HART) March 2021 report, COVID-19: an overview of the evidence, titled ‘Mortality data during the vaccine roll-out period‘ because it draws attention to a potential link between deaths in the UK’s reported second wave of COVID-19 and the vaccination roll-out amongst very vulnerable and elderly groups. We do this because, as people begin to talk more about an impending third wave, the possibility that there is a link between mortality in the second wave and the vaccination programme in the UK remains almost completely ignored. The full briefing is available here and we strongly recommend reading this key briefing (and the whole report), especially to understand the full context for the observations by Joel Smalley (who is a quantitative data analyst), below:
…. In autumn 2020, residual outbreaks started, as one would expect with viral seasonality, mostly in areas of the country that COVID-19 did not saturate in spring due to a combination of lockdowns and more remote geography. These areas were predictably hit harder in autumn/early winter 2020.
Using the modelling, region-by-region, the total expected COVID-19 excess deaths for England from October to Feb was 25,742 [see the full report – LLS]. We see 2 distinct regional ‘outbreaks’ below, in the North East and the North West (red dotted line, green dotted line) that follow a predictable course.
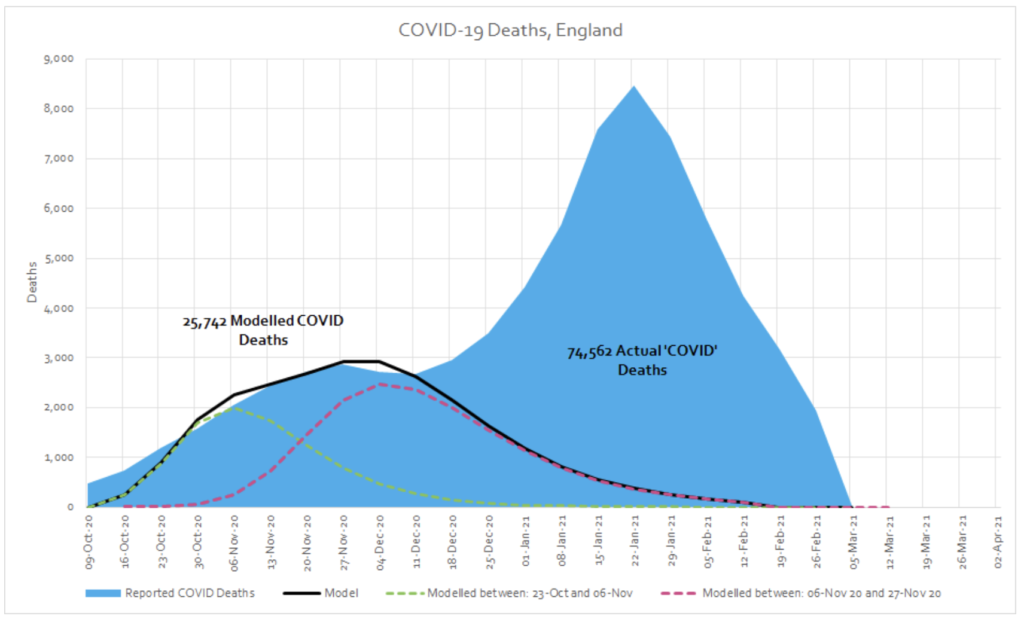
Around the second week of December a new ‘mortality series’ begins which does not fit with the pattern seen in spring or autumn. In the period from December to February, there were a total of 48,821 excess deaths (74,562 in total minus 25,742 ‘expected’ COVID-19 deaths) whose distribution is characteristically very different to spring. We would expect it to follow a similar pattern if COVID-19 was the underlying cause of this excess.
The population, demographics and the model did not change. Something new must have exerted this effect. When something in data is this unusual, we have to ask questions, no matter how uncomfortable they may be. It is an undeniable fact that this peak in deaths coincided with the mass roll-out of novel mRNA/DNA vaccines, on an extremely vulnerable population. If you compare the week ending 11 December 2020 with the week ending 29 January 2021, there was a 62% increase in total deaths and a 170% increase in COVID-19 labelled deaths in care homes.
Broken down by the separate vaccination cohort (by age group, and then taking care homes as a separate unit), the correlation between vaccination and COVID-19 deaths is even more apparent and this time the model is able to accommodate the data with significantly more ease.
This relationship is not limited to England. It is apparent in many countries around the world, regardless of location, season, interventions and extent of prior COVID-19 activity. If we include Scotland in the analysis, if winter COVID-19 excess deaths were a natural phenomenon, we would have to explain how and why it emerged first in the over 80s in England then a few weeks later in the care homes in Scotland before then jumping suddenly back to the care homes in England, before landing finally in the over 80s in Scotland.
Whilst we cannot infer causation from correlation, the mRNA/DNA vaccines had not been tested on this cohort, who have many comorbidities, multiple drug interactions and fragilities compared to trial participants and were likely particularly fragile after a year of social isolation away from loved ones. It would be extremely unscientific and even negligent not to investigate whether the rise in deaths during this period is linked in some way to the vaccine roll-out.
From a data point of view we need to ask:
● Is there a link between vaccine roll-out and a rise in cases and deaths in care homes?
● Does country by country or region by region data support or refute this possible link?
● Is follow-up data of vaccine recipients being carefully recorded for further scrutiny?
Before 2020, these would have seemed like very reasonable questions. We have entered a dangerous time where science is being censored using harmful labels like ‘anti vaxxer’. This is incredibly worrying. It is our duty as ethical scientists, and indeed citizens, to insist that these questions are properly investigated by independent bodies free of financial conflicts of interest. Indeed to date, ten countries have suspended use of the AstraZeneca vaccine amid blood clot fears.4 This recent open letter to the European Medicines Agency seems to concur that further investigation is required.5
Endnotes
1. Comparison of Growth Patterns of COVID-19 Cases through the ARIMA and Gompertz Models. Case Studies: Austria, Switzerland, and Israel
2. We shouldn’t worry when a virus mutates during disease outbreaks
3. Relation of severe COVID-19 in Scotland to transmission-related factors and risk conditions eligible for shielding support: REACT-SCOT case-control study
4. European countries suspend use of AstraZeneca vaccine over blood clot death fears
5. Urgent Open Letter from Doctors and Scientists to the European Medicines Agency regarding COVID-19Vaccine Safety Concerns
I wouldn’t normally consider myself a ‘socialist’ but I have to admit this site produces some excellent articles and analysis. Ok, I know most of the analysis comes from the work of Joel Smalley but this post breaks down the key points into nice. ‘bite-sized’ pieces. Good stuff!
As far as the politics is concerned, I’ve cone to the conclusion that the Left v Right issue is no longer relevant. When previously respected and highly regarded doctors and scientists are being silenced and intimidated by the MSM and social media there are bigger things to worry about.
Is it possible that because the vaccines reportedly produce ~10-14 days of reduced immunity after each shot, this caused an observed rise in COVID cases?
This may then be followed by a longer period – as claimed by the manufacturers – in which immunity is enhanced vs. a person who has not had COVID-19. (At the price of side effects or death in some people, hence the need to balance risks and probably not vaccinate younger or very healthy people.)
It’s abhorrent that free speech has been virtually shut down and that the three main social media are just deleting what they dislike. Private Eye started calling them anti social media some time ago … although even the Eye’s coverage of the past 15 months has been somewhat lacking.
You’re telling me! The normally sound Private Eye has, I suspect, been hamstrung by the very pro-lockdown, unquestioningly pro-vaccination stance of their MD correspondent. Their editorial line appears to be that they won’t entertain any criticism in that direction, and they have been shockingly silent on the widespread censoring of legitimate scientific and political debate on this. It makes their coverage as a whole, less than coherent to say the least!